
Why do we move or more importantly why don't we move?
When cancer treatments ends, a new chapter can start. Unfortunately, cancer survivors can still experience late effects of cancer and cancer treatment. Fear of recurrence, difficulties with focusing or physical symptoms such as fatigue or pain are a few examples.
Around 40% of cancer survivors who’ve completed treatment still experience pain. Pain that is present for longer than 3 months, is considered chronic or persistent pain. Pain has a debilitating impact on the individual, as well as having an economic and societal impact. The need for adequate pain management is obvious, the best evidence for the treatment of persistent pain in cancer survivors points to pain-education and exercise therapy.
Physical activity and exercise not only have a role in pain management but also have a positive effect on other co-morbidities such as fatigue, anxiety, depression and even a possible preventative role in cancer recurrence. Because of its benefits and low risk, it is a necessary part of treatment.
However, engaging in physical activity is a challenge. We see that exercise levels decline during treatment and that cancer survivors don’t reach their pre-diagnosis level of physical activity after ending treatment. Similarly, we see that studies with exercise interventions suffer from low adherence.
How can we help our patients in this exercise journey?
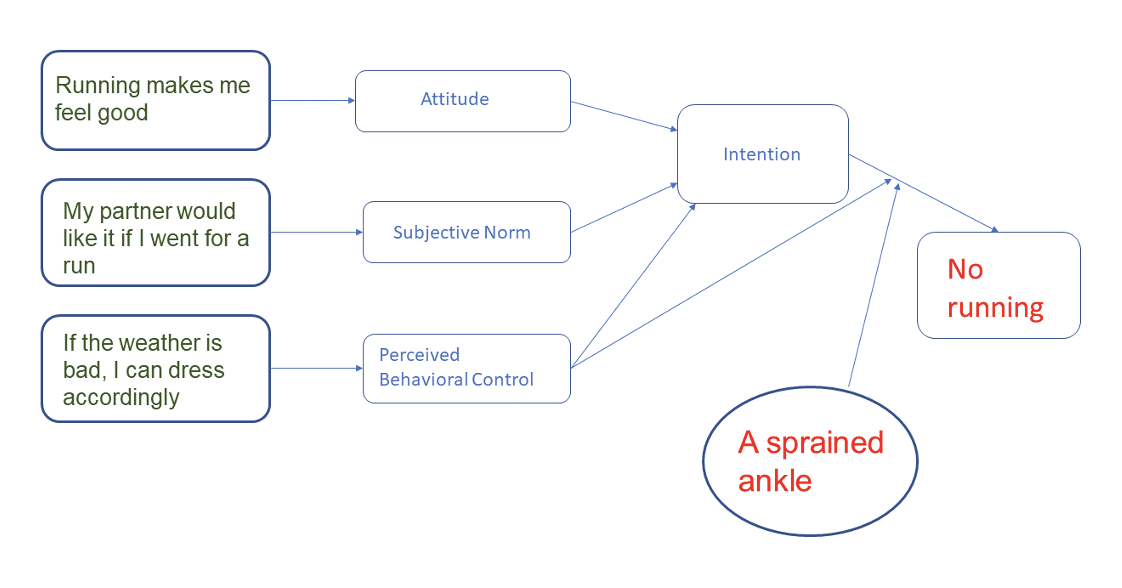
To change behavior, we must first understand what motivates behavior. Many theories of behavior and behavior change exist. A common ground is that they all incorporate biology, environment, cognition and emotion as influencing factors. To further explain behavior, we can use the theory of planned behavior of Azjen. According to this, behavior is the result of intention, perceived and actual behavioral control. The foundation of our intention is made up of the beliefs we have.
Behavioral beliefs are beliefs on the results of a particular behavior. Believing that physical activity is good for overall health or the belief that physical activity is dangerous are two examples of how a belief can positively or negatively influence behavior.
Normative beliefs are the ideas we have on the reaction of our environment. “What will my friends, colleagues or doctors think of this behavior?”, “Do they themselves present this behavior?”
Lastly, we have control beliefs: “I am too fragile to exercise”, “I don’t think I have the right skills”, “The weather is too bad to go out and exercise” “I don’t have the time for it”. Control beliefs lead to perceived behavioral control, also known as self-efficacy. Colleague Vincent Haenen wrote a great blogpost on this, so go check it out here.
All these aspects create the intention of behavior. However, a person with a true intention to exercise, can still experience barriers which hinder the actual behavior. Take a look at the following example:
When we try to change behavior, we should be aware of the interaction of all these components and try to specifically address them. So the first step is to understand these specific factors.
So, what are the beliefs, barriers and facilitators that cancer survivors experience in the uptake of physical activity? A review by Husebo et al. (2013) concluded that factors that facilitate exercise behavior are the feeling of gaining control over their health, an improvement in physical and mental well-being and social benefits. The most common barriers were treatment related side-effects, time-constraint and fatigue.
Treatment-related side-effects can encompass many symptoms and it does not offer much insight in how these side-effects actually hinder physical activity. For example in patients with chronic low back pain, the belief that pain equals tissue damage or a negative belief on resilience of their back can explain how pain can hinder physical activity.
With the knowledge that persistent pain has a high prevalence as a treatment related side-effect, a better understanding on how pain influences physical activity behavior in cancer survivors is needed. The following questions remain unanswered: what are the determinants of physical activity in cancer survivors with persistent pain and how does pain influence physical activity behavior ?
The CarEdOn research group plays an active role in the research of oncology care and wants to answer these questions, therefore we designed the Pain-DetAct study. The Pain-DetAct study aims to explore the relationships between physical activity and emotional and cognitive factors, related to pain, in cancer survivors who experience persistent pain.
Recruitement for this study will start soon so keep your eye on the CarEdOn website and social media to receive more information.
Sophie Van Dijck
References:
- De Groef A, Penen F, Dams L, Van der Gucht E, Nijs J, Meeus M. Best-Evidence Rehabilitation for Chronic Pain Part 2: Pain during and after Cancer Treatment. Journal of Clinical Medicine. 2019;8(7):979. https://doi.org/10.3390/jcm8070979
- Ajzen I. Perceived Behavioral Control, Self‐Efficacy, Locus of Control, and the Theory of Planned Behavior. Journal of Applied Social Psychology. 2002;32:665-83. https://doi.org/10.1111/j.1559-1816.2002.tb00236.x
- Husebø AML, Dyrstad SM, Søreide JA, Bru E. Predicting exercise adherence in cancer patients and survivors: a systematic review and meta-analysis of motivational and behavioural factors. Journal of Clinical Nursing. 2013;22(1-2):4-21. https://doi.org/10.1111/j.1365-2702.2012.04322.x
- Boutevillain L, Dupeyron A, Rouch C, Richard E, Coudeyre E. Facilitators and barriers to physical activity in people with chronic low back pain: A qualitative study. PLOS ONE. 2017;12(7):e0179826. https://doi.org/10.1371/journal.pone.0179826